Vol. 6 No. 1 (2024): Vol. 06 No. 1 (2024)
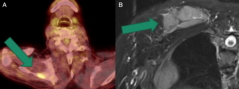
The second most common hematologic malignancy is the clonal proliferation of neoplastic plasma cells within the bone marrow. There is the presence of monoclonal immunoglobulins in the serum and/or urine. This results in anemia, myelosuppression, bone destruction, and clinical consequences of para-proteinemia on kidney function and other organ systems. The disease manifests through the acronym CRAB (hypercalcemia, renal impairment, anemia, and bone lesions). Less frequent manifestations of multiple myeloma are of extramedullary localizations. Myeloma cells can become independent of the bone marrow microenvironment, circulate freely in the blood, and infiltrate organs. This results in a high-risk state characterized by increased proliferation, evasion of apoptosis, and treatment resistance. It can affect any area of tissue. Most commonly it involves the pleura, lymph nodes, chest wall, liver, skin/soft tissue, lungs, CNS, genitourinary system, breast and pancreas. In patients with confirmed multiple myeloma, the diagnosis of extramedullary involvement is typically established by the presence of pathological soft tissue masses using radiological methods such as computed tomography (CT) scan, positron emission tomography/CT (PET/CT), magnetic resonance imaging (MRI), or ultrasound, along with biopsy or physical examination. The molecular mechanisms underlying the development of extramedullary multiple myeloma (EMM) have not been fully defined. Various cytogenetic abnormalities are observed, and some studies have generated genomic sequencing profiles that distinguish EMM from classic multiple myeloma. While plasma cell leukemia (PCL) and central nervous system (CNS) EMM indicate a poor prognosis, outcomes for other manifestations can be highly heterogeneous. Sensitive imaging modalities including PET/CT and MRI (Fig.1) are integral components of diagnosis and response assessment. Patients with extramedullary multiple myeloma (EMM) have a clear survival disadvantage.
---------------------------------------------
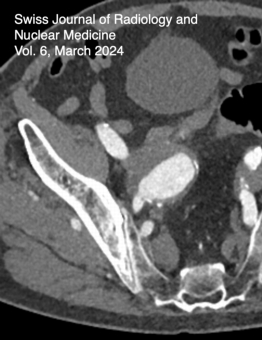
A Complex retrograde transarterial access and embolization of a giant internal iliac artery aneurysm after occlusion failure of Micro vascular plug (MVP) embolization and preceding EVAR in the distal ectatic Aorta and bilateral iliac artery aneurysmsThe therapy of pelvic aneurysms is minimally invasive through interventional radiology using various devices and embolic agents: 1. By using a covered stent/prosthesis to maintain antegrade flow when a landing zone, i.e., a vascular segment angiographically present into which the stent can be placed to bridge the neck of the aneurysm, thereby interrupting aneurysm perfusion. 2. Through complete embolization of the aneurysm using embolic agents/coils. 3. As performed in our case, by covering the aneurysm (Img 14 A-C) with a covered stent /prosthesis, following prior embolization of the branching vessels using macroembolic agents.
In cases where there is insufficient occlusion of the aneurysm with residual perfusion, secondary em- bolization becomes considerably more complex due to the occlusion of the anatomically antegrade access and the altered hemodynamics around the aneurysm causing retrograde collateralization.
Through detailed analysis of CT angiography, even in static CT, retrograde circulation could be identified, allowing for a minimally invasive secondary approach to the aneurysm without the need for general anesthesia and/or surgery. By completely eliminating the aneurysm, the risk of rupture in the elderly patient was minimally invasively eliminated. The treatment of this patient exemplifies the possibilities that embolization with a wide array of embolic agents and catheters offers in a hemodynamically very complex situation.